
| Cranial Remolding | Ni.C. Band Program | Insurance | Medical News | Deformities and Treatment | Causes | Results |
CRANIAL REMOLDING
Cranial synostosis (a fused skull suture) is a rare condition comprising less that 1% of all live births. The standard form of treatment for cranial synostosis is surgery, to release the suture and allow the skull to expand with the growing brain. Believing it to be cranial synostosis, surgeons would operate on children with Deformational Plagiocephaly. After seeing there was no fusion of the skull suture it was discovered that the soft bones of the infant skull were being deformed by their hard crib mattress.
Out of this new mandate by the American Academy of Pediatrics grew a new industry, that of cranial remolding. Cranial remolding helmets/bands (the difference between a helmet and band is the size, or lack there of, of the opening at the top) were first considered to be a class III neurologic device by the FDA. Class III devices include internal implants, artificial hearts, pace makers, devices which were surgically implanted into the body.
Papers were filed with the FDA around 1998, to demonstrate this device was more appropriately classified as a class II neurologic device. This level of classification required much less oversight by the FDA and data reporting by manufactures. The FDA subsequently created a strict set of guidelines and manufacturing standards for the production of cranial remolding devices. In the field of Prosthetics and Orthotics, only the cranial remolding band carries a class II neurological device designation.
The .PDF file below will explain cranial remolding from it's historic beginnings to present day treatment practices. We will discuss the American Academy of Pediatrics policy which lead to a near epidemic of Plagiocephaly cases, the role the FDA plays, the basic theories and principals of cranial remolding and ways in which the cranial band acts to correct and prevent further deformity.
Out of this new mandate by the American Academy of Pediatrics grew a new industry, that of cranial remolding. Cranial remolding helmets/bands (the difference between a helmet and band is the size, or lack there of, of the opening at the top) were first considered to be a class III neurologic device by the FDA. Class III devices include internal implants, artificial hearts, pace makers, devices which were surgically implanted into the body.
Papers were filed with the FDA around 1998, to demonstrate this device was more appropriately classified as a class II neurologic device. This level of classification required much less oversight by the FDA and data reporting by manufactures. The FDA subsequently created a strict set of guidelines and manufacturing standards for the production of cranial remolding devices. In the field of Prosthetics and Orthotics, only the cranial remolding band carries a class II neurological device designation.
The .PDF file below will explain cranial remolding from it's historic beginnings to present day treatment practices. We will discuss the American Academy of Pediatrics policy which lead to a near epidemic of Plagiocephaly cases, the role the FDA plays, the basic theories and principals of cranial remolding and ways in which the cranial band acts to correct and prevent further deformity.
|
|
Ni.C. Band Program
The NiC BAND Program is the only comprehensive medical treatment for improving Deformational Plagiocephaly and Brachycephaly. The eleven patient care standards set forth in the Program, detail our commitment to your child's care.
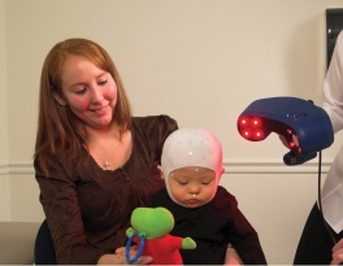
We utilize the latest Class-1 FDA approved laser data imaging system to capture a 3- dimensional image of your child's head, no plaster molding necessary. The frequent follow-up appointments necessary during cranial remolding treatment are made more convenient by our multiple office locations.
The NiC BAND Program was created to address the needs of the parent and child. Parents, having just had their infant diagnosed with Plagiocephaly, are hungry for information on the condition and its treatment. The child is in need of a safe, proven, non-invasive treatment to correct their deformity.
The NiC BAND Program is the only comprehensive medical treatment for improving Deformational Plagiocephaly and Brachycephaly. The eleven patient care standards set forth in the Program detail our commitment to you and your child. We utilize the latest Class I, FDA approved Laser Scanner to capture a three dimensional image of your infant's head.
The Laser System allows us to create a comparison of before and after treatment results, documenting the degree of correction achieved. Our dual layer foam design allows quick and accurate modification of the NiC BAND to maintain an optimum corrective environment for the skull.
The .PDF files below will detail the measurement process, Laser Scanning Technique and NiC BAND decal choices available to decorate the outside of the Band.
We utilize the latest Class-1 FDA approved laser data imaging system to capture a 3- dimensional image of your child's head, no plaster molding necessary. The frequent follow-up appointments necessary during cranial remolding treatment are made more convenient by our multiple office locations.
The NiC BAND Program was created to address the needs of the parent and child. Parents, having just had their infant diagnosed with Plagiocephaly, are hungry for information on the condition and its treatment. The child is in need of a safe, proven, non-invasive treatment to correct their deformity.
The NiC BAND Program is the only comprehensive medical treatment for improving Deformational Plagiocephaly and Brachycephaly. The eleven patient care standards set forth in the Program detail our commitment to you and your child. We utilize the latest Class I, FDA approved Laser Scanner to capture a three dimensional image of your infant's head.
The Laser System allows us to create a comparison of before and after treatment results, documenting the degree of correction achieved. Our dual layer foam design allows quick and accurate modification of the NiC BAND to maintain an optimum corrective environment for the skull.
The .PDF files below will detail the measurement process, Laser Scanning Technique and NiC BAND decal choices available to decorate the outside of the Band.
|
|

|
Insurance
The use of cranial remolding orthoses in the treatment of Deformational Plagiocephaly and Brachycephaly is considered by most insurance companies to be cosmetic in nature. Because they do not recognize the treatment as a matter of medical necessity, it is often a non-covered service. While some insurers have published criteria for approval of this service, there is no guarantee payment will be forth coming.
Our office staff will obtain all necessary prescriptions and medical necessity attestations, to file your insurance claim and seek reimbursement for you. We offer assistance in submitting appeals by providing medical literature and letter writing guidance to counter the denial reason given by the insurer.
Below are PDF files containing more detailed information on this topic.
The use of cranial remolding orthoses in the treatment of Deformational Plagiocephaly and Brachycephaly is considered by most insurance companies to be cosmetic in nature. Because they do not recognize the treatment as a matter of medical necessity, it is often a non-covered service. While some insurers have published criteria for approval of this service, there is no guarantee payment will be forth coming.
Our office staff will obtain all necessary prescriptions and medical necessity attestations, to file your insurance claim and seek reimbursement for you. We offer assistance in submitting appeals by providing medical literature and letter writing guidance to counter the denial reason given by the insurer.
Below are PDF files containing more detailed information on this topic.
Medical News
We have collected a broad range of medical literature regarding Plagiocephaly, Cranial Remolding, and matters relating to children with asymmetrical heads.
In this section we will present some of the more relevant medical articles and news issues surrounding this patient population. This information may be used for parental education, raise physician awareness of this condition and its treatment or for responding to insurance coverage denials.
At Bay Orthopedic we find an informed patient is better able to communicate issues surrounding their care and more capable and compliant with the use of their devices.
The downloadable articles are .PDF documents and will be formatted in a bibliography form with an abstract of the article.
This section will be updated frequently with new information and articles, so check back often.
We have collected a broad range of medical literature regarding Plagiocephaly, Cranial Remolding, and matters relating to children with asymmetrical heads.
In this section we will present some of the more relevant medical articles and news issues surrounding this patient population. This information may be used for parental education, raise physician awareness of this condition and its treatment or for responding to insurance coverage denials.
At Bay Orthopedic we find an informed patient is better able to communicate issues surrounding their care and more capable and compliant with the use of their devices.
The downloadable articles are .PDF documents and will be formatted in a bibliography form with an abstract of the article.
This section will be updated frequently with new information and articles, so check back often.

Deformities and Treatment
Misshapen Head Types
This section will explain cranial molding from its historic beginnings, as far back as 2000 BC, to present day treatment practices. We will discuss the American Academy of Pediatrics policy which lead to a near epidemic of Plagiocephaly cases, the role the FDA plays, the basic theories and principals of cranial remolding and ways in which the cranial band acts to correct and prevent further deformity.
There are downloads of the four main deformational skull shapes with the diagnostic signs of each condition. These documents may be given to parents, grandparents, physicians, therapists or other care givers to explain this condition and the principals surrounding its treatment.
Misshapen Head Types
This section will explain cranial molding from its historic beginnings, as far back as 2000 BC, to present day treatment practices. We will discuss the American Academy of Pediatrics policy which lead to a near epidemic of Plagiocephaly cases, the role the FDA plays, the basic theories and principals of cranial remolding and ways in which the cranial band acts to correct and prevent further deformity.
There are downloads of the four main deformational skull shapes with the diagnostic signs of each condition. These documents may be given to parents, grandparents, physicians, therapists or other care givers to explain this condition and the principals surrounding its treatment.

|
|
|
Cranial Band Treatment
The NiC BAND Program was created to address the needs of the parent and child. Parents, having just had their infant diagnosed with Plagiocephaly, are hungry for information on the condition and its treatment. The child is in need of a safe, proven, non-invasive treatment to correct their deformity.
The NiC BAND Program is the only comprehensive medical treatment for improving Deformational Plagiocephaly and Brachycephaly. The eleven patient care standards set forth in the Program detail our commitment to you and your child. We utilize the latest Class I, FDA approved Laser Scanner to capture a three dimensional image of your infant's head.
The Laser System allows us to create a comparison of before and after treatment results, documenting the degree of correction achieved. Our dual layer foam design allows quick and accurate modification of the NiC BAND to maintain an optimum corrective environment for the skull.
The .PDF files below will detail the measurement process, Laser Scanning Technique and NiC BAND decal choices available to decorate the outside of the Band.
The NiC BAND Program was created to address the needs of the parent and child. Parents, having just had their infant diagnosed with Plagiocephaly, are hungry for information on the condition and its treatment. The child is in need of a safe, proven, non-invasive treatment to correct their deformity.
The NiC BAND Program is the only comprehensive medical treatment for improving Deformational Plagiocephaly and Brachycephaly. The eleven patient care standards set forth in the Program detail our commitment to you and your child. We utilize the latest Class I, FDA approved Laser Scanner to capture a three dimensional image of your infant's head.
The Laser System allows us to create a comparison of before and after treatment results, documenting the degree of correction achieved. Our dual layer foam design allows quick and accurate modification of the NiC BAND to maintain an optimum corrective environment for the skull.
The .PDF files below will detail the measurement process, Laser Scanning Technique and NiC BAND decal choices available to decorate the outside of the Band.
|
|

|
Causes
Torticollis
Congenital Muscular Torticollis (CMT) or Wry Neck as it's called, is a disorder of the sternocleidomastoid (SCM) muscles of the neck. There are SCM muscles on each side of the neck. These muscles control rotation and tilting of the head.
In CMT, one of these muscles becomes shortened and although the exact etiology is not known, at least 40% of infants diagnosed with CMT have experienced a difficult birth. Some theorize in-utero positioning causes a contracture of one of the muscles and when the infant is placed on their back to sleep, this contracted muscle tilts and rotates the head.
Since the muscle is tight the infant yields to it and, given the infants skull is soft, the mattress their head is lying on is hard and their head does not change position, the infant develops Plagiocephaly.
Torticollis
Congenital Muscular Torticollis (CMT) or Wry Neck as it's called, is a disorder of the sternocleidomastoid (SCM) muscles of the neck. There are SCM muscles on each side of the neck. These muscles control rotation and tilting of the head.
In CMT, one of these muscles becomes shortened and although the exact etiology is not known, at least 40% of infants diagnosed with CMT have experienced a difficult birth. Some theorize in-utero positioning causes a contracture of one of the muscles and when the infant is placed on their back to sleep, this contracted muscle tilts and rotates the head.
Since the muscle is tight the infant yields to it and, given the infants skull is soft, the mattress their head is lying on is hard and their head does not change position, the infant develops Plagiocephaly.
SIDS - Sudden Infant Death Syndrome
While SIDS is not a direct cause of Deformational Plagiocephaly (DP) or Deformational Brachycephaly (DB), it is the main reason for the near epidemic of DP and DB cases we see today. A study on SIDS concluded in the early 1990's led to a policy change by the American Academy of Pediatrics (AAP).
The new policy changed the long held belief that infants were safest when placed on their stomachs to sleep. In 1992, the AAP released its recommendation that all infants be placed on their back to sleep.
Since this recommendation has been put into practice we have documented a significant rise in DP and DB cases as well as a corresponding increase in Torticollis in this population.
SIDS or Sudden Infant Death Syndrome is the sudden death of an infant under one year of age, which remains unexplained after a thorough investigation. The incidence of SIDS is currently less than one death per 1000 live births.
The Back-To-Sleep program instituted by The American Academy of Pediatricians has had a significant effect on reducing the incidence of SIDS. The program concerns placing your infant on their back when sleeping. However, the infant requires tummy time when awake to aid muscle and spine development. Tummy time should be performed when the infant is awake and a caregiver is with the child.
Below are .PDF files containing more detailed information on this condition. The files can be downloaded or printed and given to the interested party.
While SIDS is not a direct cause of Deformational Plagiocephaly (DP) or Deformational Brachycephaly (DB), it is the main reason for the near epidemic of DP and DB cases we see today. A study on SIDS concluded in the early 1990's led to a policy change by the American Academy of Pediatrics (AAP).
The new policy changed the long held belief that infants were safest when placed on their stomachs to sleep. In 1992, the AAP released its recommendation that all infants be placed on their back to sleep.
Since this recommendation has been put into practice we have documented a significant rise in DP and DB cases as well as a corresponding increase in Torticollis in this population.
SIDS or Sudden Infant Death Syndrome is the sudden death of an infant under one year of age, which remains unexplained after a thorough investigation. The incidence of SIDS is currently less than one death per 1000 live births.
The Back-To-Sleep program instituted by The American Academy of Pediatricians has had a significant effect on reducing the incidence of SIDS. The program concerns placing your infant on their back when sleeping. However, the infant requires tummy time when awake to aid muscle and spine development. Tummy time should be performed when the infant is awake and a caregiver is with the child.
Below are .PDF files containing more detailed information on this condition. The files can be downloaded or printed and given to the interested party.
Environmental Causes
The factors causing Deformational Plagiocephaly and Deformational Brachycephaly are many. The primary reason for the rapid increase in this condition can be traced back to 1992. A study of newborns showed that infants who slept on their backs had a significantly lower incidence of Sudden Infant Death Syndrome (SIDS).
The dramatic drop in SIDS cases reported in this study resulted in a change in the recommended sleeping position of infants by the American Academy of Pediatrics. No longer would the AAP recommend infants sleep on their stomachs. A campaign was launched called the “ Back To Sleep Campaign”. Parents are being instructed to place their infants on their back to sleep.
However, the second part of the Back To Sleep Campaign is to place your infant on their stomach when they are awake and you are with them. Many parents fail to hear this part and have their infants on their back all the time.
Please see the .PDF document below for more information on this topic.
The factors causing Deformational Plagiocephaly and Deformational Brachycephaly are many. The primary reason for the rapid increase in this condition can be traced back to 1992. A study of newborns showed that infants who slept on their backs had a significantly lower incidence of Sudden Infant Death Syndrome (SIDS).
The dramatic drop in SIDS cases reported in this study resulted in a change in the recommended sleeping position of infants by the American Academy of Pediatrics. No longer would the AAP recommend infants sleep on their stomachs. A campaign was launched called the “ Back To Sleep Campaign”. Parents are being instructed to place their infants on their back to sleep.
However, the second part of the Back To Sleep Campaign is to place your infant on their stomach when they are awake and you are with them. Many parents fail to hear this part and have their infants on their back all the time.
Please see the .PDF document below for more information on this topic.
Results
Before and After
Cranial Remolding through the use of a Band or Helmet is a proven corrective treatment. Scientific literature exists showing the benefits of prescribed use of the Band or Helmet. In articles published by S. Clarren, MD, Ripley and Pomatto, Mulliken and others, all demonstrate the corrective influence of cranial remolding.
Factors that can influence the degree of correction include; starting age of the infant, the degree of asymmetry of the skull, the infants growth rate among others. In cranial remolding, the younger the patient the patient starts treatment the better. Average starting age is 6 months of age, although 4 months old would be better. The most rapid period of growth is between birth and 8 months of age. Good growth exists between 8 and 12 months of age but, after 12 months of age growth slows significantly.
The second factor, the degree of asymmetry, factors greatly into the equation when compared to starting age. While there is no published scale for quantifying severity, an accepted formula for gauging pathological head shape has been created. A ratio called the Cephalic Index, which is calculated by dividing the width of the head by its length. Normal is considered to be 78%, while pathological flathead (back to sleep head shape) is in the range of 85% to 100%. Scaphocephaly or narrow head shape is in the 60 to 70% range.
The third most common factor influencing the degree of correction is the baby's own growth rate. The head circumference, length, and weight of an infant change monthly. If the baby's head grows slowly correction often takes longer and is less dramatic. Brain growth rate is greatest when children are between birth and 8 months old. This is the reason we want to start cranial remolding early, to capture the rapid brain growth.
Please view the .PDF files for some dramatic results of NiC BAND Program.
Before and After
Cranial Remolding through the use of a Band or Helmet is a proven corrective treatment. Scientific literature exists showing the benefits of prescribed use of the Band or Helmet. In articles published by S. Clarren, MD, Ripley and Pomatto, Mulliken and others, all demonstrate the corrective influence of cranial remolding.
Factors that can influence the degree of correction include; starting age of the infant, the degree of asymmetry of the skull, the infants growth rate among others. In cranial remolding, the younger the patient the patient starts treatment the better. Average starting age is 6 months of age, although 4 months old would be better. The most rapid period of growth is between birth and 8 months of age. Good growth exists between 8 and 12 months of age but, after 12 months of age growth slows significantly.
The second factor, the degree of asymmetry, factors greatly into the equation when compared to starting age. While there is no published scale for quantifying severity, an accepted formula for gauging pathological head shape has been created. A ratio called the Cephalic Index, which is calculated by dividing the width of the head by its length. Normal is considered to be 78%, while pathological flathead (back to sleep head shape) is in the range of 85% to 100%. Scaphocephaly or narrow head shape is in the 60 to 70% range.
The third most common factor influencing the degree of correction is the baby's own growth rate. The head circumference, length, and weight of an infant change monthly. If the baby's head grows slowly correction often takes longer and is less dramatic. Brain growth rate is greatest when children are between birth and 8 months old. This is the reason we want to start cranial remolding early, to capture the rapid brain growth.
Please view the .PDF files for some dramatic results of NiC BAND Program.
Computer Comparison
Bay Orthopedic and Rehabilitation Supply has invested in the latest Laser Imaging System for Prosthetics and Orthotics. The Class I laser is eye safe and allows movement of the body part being scanned. This allowance for movement makes this system superior over others for cranial remolding.
The computer software allows for an infinite number of views of the scanned head. This is particularly well suited for comparison of before and after treatment results and for insurance company outcome reports. The software also has the ability to calculate differences in measurements of the before and after scans.
Another feature of the comparison software is the creation of an overlay image. The initial scan and final scan are oriented and laid over one another. The computer produces an outline of the two images superimposed over each other. The superimposed image clearly shows the correction achieved from the NiC BAND Program.
Below are .PDF files showing these images and the overlay comparison.
Bay Orthopedic and Rehabilitation Supply has invested in the latest Laser Imaging System for Prosthetics and Orthotics. The Class I laser is eye safe and allows movement of the body part being scanned. This allowance for movement makes this system superior over others for cranial remolding.
The computer software allows for an infinite number of views of the scanned head. This is particularly well suited for comparison of before and after treatment results and for insurance company outcome reports. The software also has the ability to calculate differences in measurements of the before and after scans.
Another feature of the comparison software is the creation of an overlay image. The initial scan and final scan are oriented and laid over one another. The computer produces an outline of the two images superimposed over each other. The superimposed image clearly shows the correction achieved from the NiC BAND Program.
Below are .PDF files showing these images and the overlay comparison.


|

|
